1. What is the mechanism of action of opioids?
Analgesia: μ-receptor agonism in brain (periaquaductal gray matter) and spinal cord (substantia gelatinosa). Opioids bind to G-Protein-coupled opioid receptor and inhibit adenylate cyclase and voltage gated Calcium channels. This reduces excitability and interferes with pain transmission.
2. What are the different types of opioid receptors and the effects at these receptors? Where are they located?
Side effects:
μ-receptor agonism:
- Constipation due to ↓GI Transit.
- Pruritis
- Urinary Retention
- Biliary Spasm
μ1 receptor agonism:
- Prolactin release.
μ2 receptor agonism:
- Respiratory depression
- Bradycardia
- Hypotension
- Constipation due to ↓GI Transit.
K receptor agonism:
- Sedation
- ↓ADH Release
δ receptor agonism:
- Respiratory depression
- Constipation due to ↓GI Transit.
- Growth hormone relase
- Urinary retention.
δ2 receptor agonism:
- Pupillary constriction, nausea, vomiting.
3. What are the advantages of neuraxial opioids vs. intravenous opioids?
| Neuraxial Opioids | Intravenous Opioids | |
|---|---|---|
| + Selective Effects | - Systemic Side Effects | |
| + Reduction in systemic complications | + Can be quickly reversed with Naloxone. | |
| + Dose-sparing effect | ||
| - Side effects may be more sudden and severe | ||
| - Side effects may be more difficult to reverse. |
4. What are the side effects of neuraxial opioids?
- Side Effects of Neuraxial Opioids:
- Hypotension (abrupt pain relief → decreases adrenaline)
- Pruritis (unclear etiology)
- Urinary Retention (inhibition of sacral parasympathetic flow → Detrusor Relaxation)
- Early Respiratory Depression (systemic absorption)
- Late Respiratory Depression (migration to medulla).
- Nausea/Vomiting (rostral migration to chemoreceptor trigger zone)
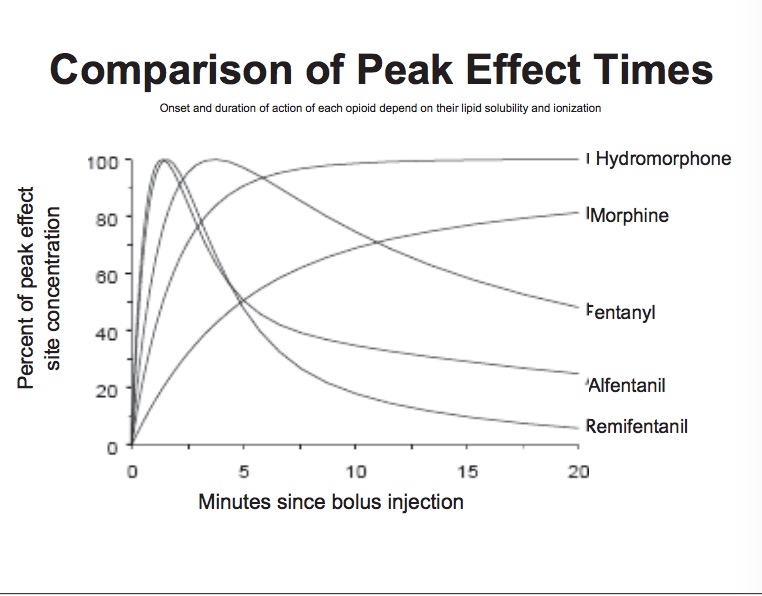
List the commonly used opioid agonists and there relative potencies, pharmacokinetics and side effects.
-
Morphine
- Relatively low potency
- Active Metabolite, morphine-6-glucuronide has analgesic properties and is renally extreted.
- Can cause histamine release (Pruritis and Vasodilation)
-
Hydromorphone (Dilaudid)
- 8x more potent than morphine.
- No active metabolites, no histamine release.
-
Fentanyl
- 100x more potent than morphine.
- Fast onset and short duration of action.
- Unlike morphine, no histamine release, so does not cause vasodilation and hypotension.
- Causes more intense respiratory depression compared to morphine.
- Causes less nausea compared to moprhine.
-
Remifentanil
- 200x more potent than morphine
- Extremely rapid offset (~90 sec) as it is metabolized by plasma esterases (as opposed to the liver).
5. Which opioid antagonist is most commonly used and how is it dosed?
Naloxone (Narcan) can be used to reverse the effects of opioids. It is a competitive antagonist for central opioid receptors.
Dosing: 0.40mg – 2mg IV q2 minutes. (Can dilute to give in 0.04mg increments)
If no response after 10 mg, reconsider narcotic overdose as cause of delayed emergence.
Narcan's effects last for ~45 min. It should be given with caution, as pain control becomes difficult to achieve after narcan is administered.