Central Venous Catheter
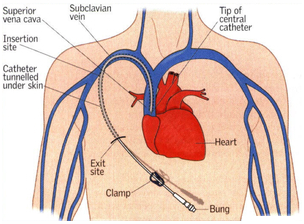
- Sits in subclavian or internal jugular with tip directed towards SVC.
- Measures RAP RVEDP = RV preload and thought to parallel LAP and thus LV preload.
- Inaccurate in ptatients with pulmonary HTN, Right heart disease, valvular pathologies, pulmonary edema, PEEP (↑ intrathoracic pressure during expiration ↑ CVP)
- Also used to infuse inotropes or vasopressors
Causes of Preoperative Volume Loss
- Vomiting
- Diarrhea
- Fever
- Sepsis
- Trauma
- Fluid shifts (e.g. burns, ascites, pleural effusion)
Intraoperative Volume Assessment
Not very reliable:
- HR and BP (control for PPV and anesthetics may cause relative hypovolemia)
- Pulse Oximetry (waveform wanters from baseline)
- Urine Output (stress response from surgery increases ADH so not reliable measure).
- Serial ABGs to check lactate.
Reliable in the absence of heart pathology
- Central Venous Catheter (for CVP).
Very reliable:
- Pulmonary artery catheter: Most commonly used for in RV dysfunction, pulmonary hypertension, valvular pathology (AS, MR), LV dysfunction.
- Transesophageal Echocardiogram: Commonly used in major cardiac surgeries and liver transplants.
Intraoperative Fluid Requirements
Maintenance: Generally 4-2-1 rule used. 4ml/hr/kg for first 10 kg, 2 ml/hr/kg for next 10 kg, 1 ml/hr/kg for each additional kg.
Compensation for pre-existing fluid defecits: Multiply maintenance requirements by the number of hours NPO. Give 1/2 of additional fluids in the first hour, 1/4 in the 2nd hour, and 1/4 in the 3rd hour.
Example:
For a 70 kg man, the total fluid requirements are 4 x 10 kg + 2 x 10 kg + 1 x 50 kg = 110 ml/hr.
If the man has been NPO for 8 hours, he needs an additional 880 ml (for a total of 990 ml). 440 ml (on top of the maintenance 110 ml) will be given in the first hour of the surgery. 220 ml (+110 ml maintenance) will be given in each of the next two hours).
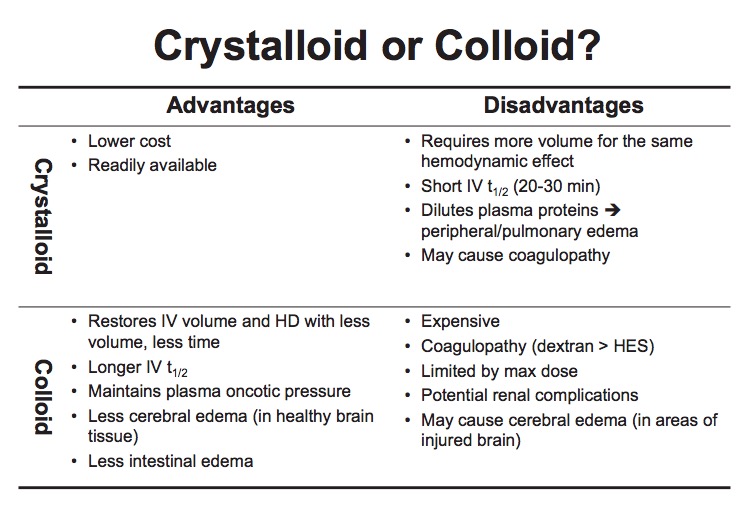
Types of Fluid